The disclaimer
Well, I haven’t squeezed the flannel dry on this topic. Just a heads up that if you are not into running this blog, like the flannel, will be dry. All this advice is based on my experiences so you’ll need to individualise it. Want to know more about my experience running the marathon click this.
The intro
When you think about it a marathon is an unreasonable distance for anyone to run continually. 42.195km is an unpleasant looking thing, I mean, just round it down to 42! In training I have frequently asked myself the question: why? You’ll also recognise this question if you have ever experienced hitting the wall. It’s a personal pain dungeon. The marathon is masochism on a grand scale, but then again isn’t that the appeal? And nothing’s worth doing unless it’s a challenge, right? At least that’s what you tell yourself.
The wall
In all my previous marathons I have hit the wall. It is like nothing else: tunnel vision, extreme fatigue, brain fog, just the sound of your rasping breath and the road curling up inception-like in front of you. You can’t even muster a grimace ‘cos your face has inexplicably melted! The Dutch have coined it nicely, the man with the hammer. The scourge of all runners. So for those of you who are interested in how I trained for sub 3, this time with no sign of the wall, here is my framework. This was my minimum amount of training needed, so probably not wise to do any less than this, unless you’re borderline Kipchoge:

- Starting level: a recent 38:30 min 10km, or an 19:00 min 5k.
- Runs per week: 3
Every run has a certain goal and specificity. No album fillers. This means the runs themselves are tougher, but you have longer recoveries, which is particularly important if you are over 30. - Rest days per week: 3
In my experience most training plans don’t allow enough rest days. There are some I have seen online that give 6 runs a week. This is totally unsustainable in my book and will cause injuries. As a physio, I see this all the time. - Swims per week: 1 (recovery/cross-training after intervals)
- Build-up per week: 10%
A 5-10% increase is the physical maximum adaptation per week (decreases with age)
The specifics
Below is an outline of my training schedule:
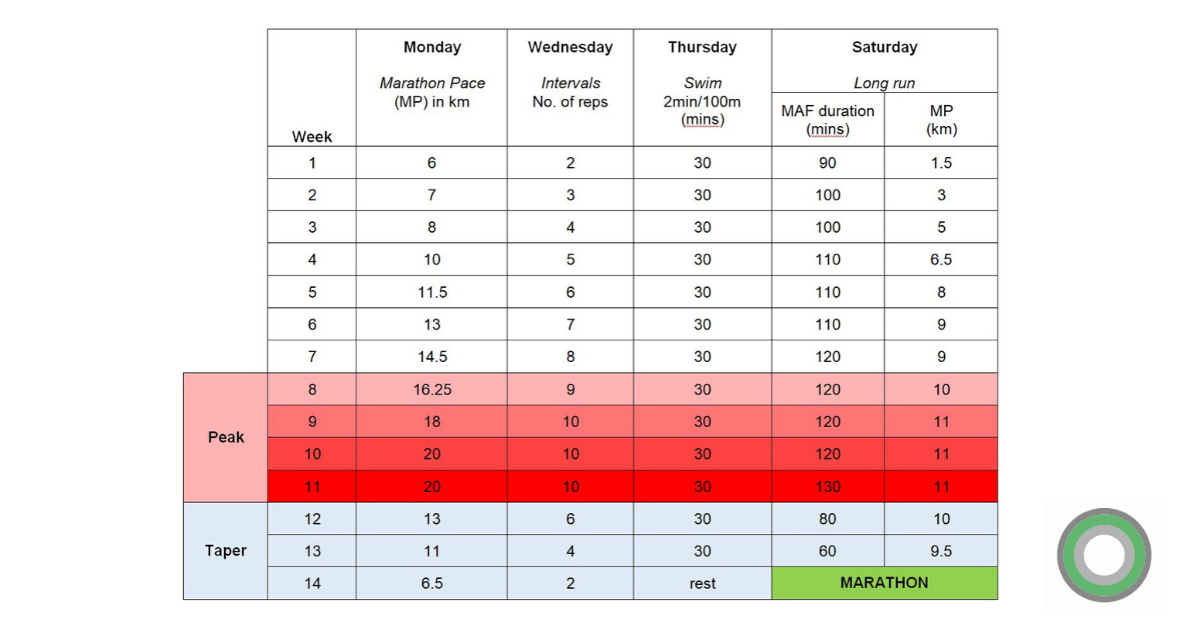
Monday: Marathon Pace (MP) – 4:15/km
Simple marathon pace runs for increasingly long distances. Approaching the marathon, your body is absolutely attuned to this pace and you’ll be able to run this pace probably without even looking at the watch, you’ll just know how it feels. Don’t worry if you feel like it never seems to get easier, during tapering your body will adjust and come marathon day it’ll feel much easier.
Measure your heart rate (HR) on the first of these runs and you will see small reductions in HR at the same pace, throughout the 14 weeks. As a loose guide it is said that you can’t maintain more than a 165 bpm HR average over a 3 hour marathon. If in the marathon you’re already tipping into the 170s at the half way point, you’ve probably over-cooked it, and will be found out.
Wednesday: Track intervals – 800m at 3:40/km (fast pace) with 400m slow recovery laps
This increases heart stroke volume: volume of blood pumped in one pump, i.e. the power of the heart muscle. Progress in cardiovascular efficiency will occur as your lactate threshold improves.
Thursday: Recovery swim – 30 mins
I am a terrible swimmer so 30 mins is a big cardio effort for me – 2 min/100m was enough for me to maintain a hard cardio effort, with no strain on the joints. Also a 20 min hard cycle to and from the swimming pool, keeps a good 60 or so mins cardio effort.
Saturday: Long run – up to 3 hours
This run is absolutely crucial. I have skipped some of these in the past and not managed under 3 hours as a result. If you must skip a training session, skip one of the other runs. These runs generate aerobic and metabolic adaptations that are absolutely vital if you want to go sub 3.
This run has 2 sections:
- MAF (Max Aerobic Function) running based on running at heart rate of up to 145 bpm (MAF is loosely 180 bpm minus your age). This is held for an increasing amount of time running every week (up to max of 2 hours 10) followed immediately by MP. It should feel relatively easy, if it doesn’t, go slower. I would sip up to 300ml water slowly in section 1, based on a temperature of around 10 degrees or lower.
- Marathon pace (4:15/km). This is to simulate race conditions creating an up to max heart rate effort at the point of fatigue, like the end of a marathon. For me these were by a long way the hardest runs. Done without nutrition in the MAF section, only allowing one gel at the beginning of section 2 means your body becomes used to metabolising the calories at marathon pace and at fatigue, but also increases your glycogen stores as you essentially starve your body of energy up until this point. I used Powergel Smoothies from PowerBar (65% fruit puree, with electrolytes). They’re easy to digest in combination with standard gels. Don’t try a new one for the race, try a few on your long training runs.
So that’s it, 4 different activities, on loop for 14 weeks. Boring, but effective. Get your podcasts on.
Peak training period (weeks 8-11)
Fatigue and recovery are affected by multiple external conditions- sleep, nutrition, footwear, stress to name a few. Don’t plan too much in outside of work, you’ll be knackered. Eat well, sleep well and keep the avoidable stresses to a minimum.
In the early training weeks I would increase all three runs each week, while in weeks 8-11 I increased only one or two of the three runs each week. Here you are dealing with the most accumulated fatigue and are working regularly at your physiological limit, so it is an injury tightrope. One or two sessions will feel unexpectedly horrendous, don’t be scared to cut it short in this case, your body is telling you something and one shortened/slower run won’t hurt.
Do not play any other sport in this period – explosive high energy sport is likely to irritate tendons that are being put under a lot of stress with the training. As a rule, I would avoid any other sporting activities that aren’t in the training plan.
The taper
Tapering begins 3 weeks from the marathon, but I added a few easy-paced 3 hour recovery cycle rides to give the running joints a rest and sustain the 3 hour cardio efforts until the last week of tapering, where I did next to no running and no cycling to gain full advantage of the body’s adaption period during a taper.
Do not be tempted to over-train when tapering. Your body is recovering, so let it recover. Some training plans begin the taper at 4 weeks out, this is too early for me. I tried it, and it didn’t work. Looking at the consensus in the literature, the longest run should be 3 weeks before the marathon.
Next post will be on training and race nutrition, so stay tuned.




 One of the biggest consequences of life today is that we don’t need to move. Work for a huge amount of us involves sitting at a desk all day long in front of a computer or looking down at our smart phones. I include myself in this. Although my job involves a hands-on aspect treating people I still find myself spending more and more time in front of a computer because of the demands of running a business as a physiotherapist. We cannot always change the fact we have to work like this but we can alter how we counteract the prolonged periods of being sedentary.
One of the biggest consequences of life today is that we don’t need to move. Work for a huge amount of us involves sitting at a desk all day long in front of a computer or looking down at our smart phones. I include myself in this. Although my job involves a hands-on aspect treating people I still find myself spending more and more time in front of a computer because of the demands of running a business as a physiotherapist. We cannot always change the fact we have to work like this but we can alter how we counteract the prolonged periods of being sedentary. 
 I spend a lot of time treating muscles because they can be the source of a lot of patient’s problems. This is because they have such a key role within the body and we ask so much of them. There are 3 types of muscle: skeletal (they move parts of the body including arms and legs), smooth (found in the internal organs) and cardiac (heart). Today I thought I would discuss skeletal muscle.
I spend a lot of time treating muscles because they can be the source of a lot of patient’s problems. This is because they have such a key role within the body and we ask so much of them. There are 3 types of muscle: skeletal (they move parts of the body including arms and legs), smooth (found in the internal organs) and cardiac (heart). Today I thought I would discuss skeletal muscle. Lower back pain is one of the most common problems I see in my practice. The severity, duration and intensity is variable but the predominant reason for patients attending physiotherapy is the same. They are in pain and the pain is affecting their daily lives and ability to carry out activities.
Lower back pain is one of the most common problems I see in my practice. The severity, duration and intensity is variable but the predominant reason for patients attending physiotherapy is the same. They are in pain and the pain is affecting their daily lives and ability to carry out activities. Often, when it is someone’s first time attending a physiotherapy assessment they do not know what to expect. I thought I would write a brief blog outlining the fundamentals of a physiotherapy assessment in the practice setting and how the assessment determines what treatment comes next.
Often, when it is someone’s first time attending a physiotherapy assessment they do not know what to expect. I thought I would write a brief blog outlining the fundamentals of a physiotherapy assessment in the practice setting and how the assessment determines what treatment comes next. There is quite a varied opinion on what physiotherapy is and what physiotherapists do. This is not surprising as people’s opinions will depend on their own experiences with physiotherapy which can be very different depending on why they required the physiotherapy in the first place. Physiotherapists can be found throughout all aspects of healthcare. From Intensive care rehabilitation, stroke units, children’s wards to a general practice on the high street.
There is quite a varied opinion on what physiotherapy is and what physiotherapists do. This is not surprising as people’s opinions will depend on their own experiences with physiotherapy which can be very different depending on why they required the physiotherapy in the first place. Physiotherapists can be found throughout all aspects of healthcare. From Intensive care rehabilitation, stroke units, children’s wards to a general practice on the high street.